Dunnington Gl The Art of Mentoring Am J Surg 19961716604607
D Mulholland1, G McEnteeone, C Quinlan3, R McDermottiv, N Foley1, N Hogan5, A Hogan2
1Mater Misericordiae University Infirmary, Eccles St, Dublin 7
2Mayo General Hospital, Castlebar, Co Mayo
3St Vincent's University Hospital, Elm Park, Dublin 4
4St James'southward Infirmary, James's St, Dublin viii
fiveClinical Science Institute, NUI, Galway
Abstract
A significant amount of valuable undergraduate medical educational activity may be informal, unscheduled and delivered by non-consultant hospital doctors (NCHDs). 800 Questionnaires were distributed to consultants, NCHDs and medical students in Irish educational activity hospitals. The aim was to quantify the level of unscheduled pedagogy carried out in these hospitals and the mode in which information technology was performed. The response rate was 46% (364/800). 71% of doctors who replied are independently teaching undergraduate medical students (77/109), including 71% of interns and senior house officers (48/68). Students tend to adopt minor group teaching. 50-half dozen percentage of students suggest they would do good from more surgical instruction fourth dimension (144/255). No interns surveyed were scheduled to teach equally office of a formal curriculum. A significant amount of unscheduled instruction by interns and senior business firm officers takes place in Irish gaelic hospitals. It may prove beneficial to comprise interns into scheduled surgical instruction curricula.
Introduction
Undergraduate education has a powerful effect on medical students, influencing not merely grades1, simply as well career optionii and enjoyment of surgical rotations3. It has been shown that the level of involvement in surgery is declining4 and that resident staff who are effective educators and mentors encourage students to pursue surgical careers2. Pedagogy is beneficial for business firm officers equally it increases their own medical knowledge5. While carefully constructed curricula are in place, a neat deal of surgical teaching is unscheduled and entirely dependent on the consultant or non-consultant hospital doctor (NCHD) involved. These encounters tend to be brief, ad hoc and unplanned6. This informal teaching even so, has the potential to have a positive impact on medical students' experience of surgery. Information technology has been suggested that junior infirmary staff are more crucial to the undergraduate learning experience than consultants, every bit much of the onus of teaching medical students, particularly in the area of perioperative direction falls to the NCHDsthree.
The nowadays study attempts to quantify the amount of unscheduled didactics provided by surgical NCHDs and consultants in Irish didactics hospitals, and to establish potential for comeback. Interns are in their first twelvemonth mail service-qualification, Senior Firm Officers typically two and iii years post-qualification, with Registrars and Tutors typically four to six years and Specialist Registrars greater than 5 years post-qualification. The secondary aim was to examine the teaching medium with which surgeons and trainees feel almost comfortable. The tertiary aim was to assess students' experiences with unscheduled teaching and to assess their ranking of teachers of different grades.
Methods
250 questionnaires were distributed over a 3 calendar month period to NCHDs and consultants working in seven Irish Academy Hospitals, each a tertiary referral centre with large numbers of undergraduate students attending annually. A total of 550 surveys were distributed to medical students at the end of their preparation in all major tertiary-level institutions in Ireland. Students were asked to rate which style of didactics they found to be most useful, once again using a 5-signal Likert scale with 1 beingness the most beneficial and 5 being the to the lowest degree beneficial. The modes of instruction investigated were didactic tutorials, bedside tutorials, case presentations, lectures and information interpretation sessions. Post-obit retrieval of the completed questionnaires the results were tabulated and analysed (Tables one and two).
Results
Survey 1
A full of 109/250 (44%) surveys were completed by various grades of hospital doctors - interns (45), SHOs (23), Registrars (10), Specialist Registrars (xiii), Surgical Tutors (4) and Consultants (14).
Scheduled Teaching
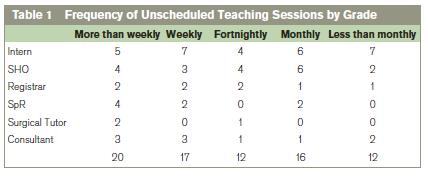
64% (lxx/109) of responders were not scheduled to provide undergraduate teaching. No intern was scheduled to teach as part of the formal undergraduate curriculum compared to 22% (5/23) of SHOs and 83% (34/41) of registrars, tutors, specialist registrars and consultants. The almost common form of scheduled didactics was bedside tutorials 42%, (22/53), followed by didactic tutorials 28% (15/53), with 17% (9/53) scheduled to deliver formal lectures, 11% (6/53) scheduled to hear instance presentations and 1% (one/53) scheduled to deliver information interpretation sessions.33% (13/39) responders were scheduled for more than than one instruction session per week with 53% (21/39) scheduled for weekly sessions. The remaining 12% (5/39) had been scheduled for fortnightly or less frequent sessions.
Unscheduled Teaching
71% (77/109) respondents provided unscheduled pedagogy sessions, 64% of Interns (29/45), 83% of SHOs (nineteen/23), eighty% of Registrars (8/10), 69% of Specialist Registrars (9/13), 75% of Surgical Tutors (3/4) and 64% of Consultants (9/14) provided unscheduled teaching to undergraduates.The most common style of unscheduled teaching was bedside tutorials 39% (48/124), followed by didactic tutorials 25% (31/124) and case presentations 24% (thirty/124). But a small minority provided unscheduled lectures or data interpretation sessions, 12% (15/124).With regards to frequency of the unscheduled sessions, 64% of responders (49/77) providing unscheduled education sessions did so on at least a fortnightly footing (Table 1).
Miscellaneous
33% of (36/109) responders reported adequate time to teach, 33% of interns (15/45), 17% of SHOs (4/23), 40% of registrars (4/10), 38% of Specialist Registrars (5/13) and 35% of Consultants (5/13). 87% surveyed (94/109) could provide fortnightly or more than sessions with 14% (15/109) stating they could only teach monthly or less than monthly.75% (39/52) of interns and SHOs reported bedside tutorials (17/52) or didactic tutorials (23/52) as their preferred fashion of teaching and 85% reported lectures and data interpretation sessions as the to the lowest degree preferred (44/52).
Survey 2
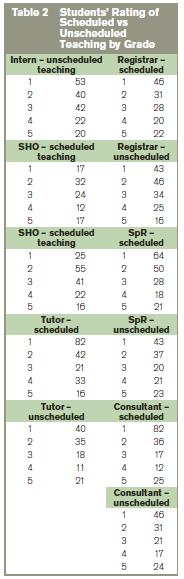
A total of 184 surveys were fully completed and 71 were partially completed by medical students throughout the country.56% of students felt they were not receiving enough educational activity (144/255). 87% felt they would do good from more scheduled educational activity fourth dimension (221/255). 67% of students (142/255) received unscheduled teaching sessions on a weekly footing and 36% received at least twice weekly sessions (91/255).Students' rating of scheduled and unscheduled educational activity performed by each rank of doctor from intern to consultant is shown in Table ii. 63% of students rated bedside tutorials as the about beneficial mode of pedagogy (132/184).
Give-and-take
While the numbers of doctors (109/250) and students (255/550) who replied were less than 50% in both cases this written report suggests that in Ireland, a minority of surgeons (consultants and trainees) are scheduled for formal teaching sessions every bit part of the undergraduate curriculum. These scheduled pedagogy sessions consist mainly of small group teaching, including didactic tutorials and bedside didactics. The latter was the mode of teaching virtually preferred by teachers and students alike, but such sessions are limited as simply small numbers of students tin can nourish. In order to provide adequate pedagogy to all students, more tutors are required. The final years of medical undergraduate educational activity are characterised by various in-hospital placements with unlike specialist teams. This 'clinical apprenticeship' provides opportunities to practice clinical skills under the watchful center of experienced clinicians who provide constructive feedback and gradually relax their level of intervention equally the students become more proficient7. This clinical clerkship is the primary source of mentoring, or form of apprenticeship8.
However, with decreasing numbers of constituent surgical admissionsnine and increasing numbers of long stay patients10,11, the opportunities for medical students to acquire has become more express. Such long term patients are less suitable for teaching and learning the basics of history taking, physical examination, and clinical evaluation as their acute illness has resolved. Clinical skills are disappearing12, the availability of pupil mentors has decreased drastically13 and traditional bedside teaching skills have deteriorated as each generation is less exposed to themxiv. Our study suggests that a pregnant amount of unscheduled education takes place within surgical teams. The inferior members of the team are contributing significantly to such teaching and this teaching is valued by the students. Despite this, students feel they are not getting plenty teaching in surgery. Small group educational activity is the preferred mode of pedagogy for students and teachers alike and the majority of teachers feel they could commit to fortnightly or greater teaching sessions for undergraduates. Junior members of the surgical squad should be treated as a valuable pedagogy resource as they themselves accept experienced final medical exams more recently than whatever other grade of doctor.
Past incorporating interns and SHOs into formal educational activity curricula the number of pocket-size group and bedside tutorials could increase. Such a policy shift would also increase the number of pupil mentors available which may augment the clinical skills and expand the medical noesis of our undergraduate students. In addition, it may upskill didactics skills among future generations, equally more students volition have augmented exposure to traditional bedside teaching. More regular mentoring may also assistance to counteract the declining numbers of junior hospital doctors interested in a surgical career15. Every bit interns and the vast majority of SHOs are currently non scheduled to teach, information technology is reasonable to assume that they could conceivably be incorporated into existing curricula in order to provide extra small group instruction for undergraduates. This should confer greater benefits for both students and teachers alike2,5,vi.
Correspondence: D Mulholland
Mater Misericordiae University Hospital, Eccles St, Dublin 7
Email: [email protected]
References
1. Langenfeld SJ, Helmer SD, Cusick TE, Smith RS. Do Strong Resident teachers Help Medical Students on Objective Examinations of Knowledge? J Surg Educ 2011 Sep-Oct;68:350-4.
2. Musunuru S, Lewis B, Rikkers LF, Chen H. Effective Surgical Residents Strongly Influence Medical Students to Pursue Surgical Careers J Am Coll Surg, 2007;203:164-7.
iii. Whittaker LD Jr, Estes NC, Ash J, Meyer LE. The value of resident teaching to amend student perceptions of surgery clerkships and surgical career choices Am J Surg 2006 Mar;191:320-4
4. Arnold MW, Patterson AF, Tang L. Has implementation of the 80-60 minutes work week made a career in surgery more highly-seasoned to medical students? Am J Surg 2005;189:129–133.
5. Chamberland Thousand, Boulé R. Residents and the education role: review of the literature. CMAJ 1990 Oct 15;143:725-xxx.
half dozen. Jeffree RL, Clarke Air conditioning. X Tips for Teaching in the Theatre Tearoom: Shifting the Focus from Education to Learning Earth J Surg 2010 34; 2518-23.
seven. Ashley EA. Medical Education – beyond tomorrow? Medical Education 2000;34:455-nine.
8. Lewis T. The youngest scientific discipline; Notes of a medicine-watcher. The Viking Press. New York. 1983.
nine. Robb WB, O'Sullivan MJ, Brannigan AE, Bouchier-Hayes DJ. Are constituent surgical operations cancelled due to increasing medical admissions? IJMS 2004; 173:129-132
10. Costa AP, Poss JW, Peirce T, Hirdes JP Acute care inpatients with long-term delayed- discharge: bear witness from a Canadian health region. BMC Health Services Inquiry 2012, 12:172
11. P Gallagher, Due north O'Callaghan, C Henry. Exercise Relatives of Elderly Patients Block the Discharge Process? IMJ 2012;105:5
12. Dunnington GL. The art of mentoring. Am J Surg 1996;171:604-7.
xiii. Mangione S, Nieman LZ. Cardiac auscultatory skills of internal medicine and family exercise trainees. A comparison of diagnostic proficiency. JAMA 1997;278:717-22.
xiv. Ramani S, Orlander JD, Strunin Fifty, Barber TW. Whither bedside education? A focus-group study of clinical teachers. Acad Med 2003; 78: 384-90.
15. Erzurum VZ, Obermeyer RJ, Thyagarajan P, Tan P, Koler AK, Hirko MK, Rubin JR. What influences medical students' option of surgical careers Surg 2000; 128: 253-256.
| Author's Correspondence |
| No Writer Comments |
| Acknowledgement |
| No Acknowledgement |
| Other References |
| No Other References |
0 Response to "Dunnington Gl The Art of Mentoring Am J Surg 19961716604607"
Post a Comment